
Summary:
- We describe a case of severe Covid-19 (a man of advanced age and multiple comorbidities including diabetes mellitus, hypertension, obesity and active chronic hepatitis B) who improved quickly upon receiving the “Integrative antioxidant” intervention” approach and was discharged from hospital 4 days after the implementation of the approach.
- Severe/critical cases of Covid-19 cases are characterized biochemically and pathologically by cytokine storm with rapidly rising oxidative stress, leading to severe oxidative damage of biologically important macromolecules, cells, and eventually multiple organ failure and death.
- Early, sufficient doses and integrative antioxidants administration, to block or reduce oxidative stress, cytokine storm, may be able to prevent or reduce the oxidative damages of biologically important macromolecules (especially poly-unsaturated fatty acids in bio-membranes, PUFA, lipid peroxide chain reaction) and multi-organ failure, death.
- The optimal efficiency of our body’s antioxidant systems requires all components to be present and in sufficient amounts. Inadequate or absent of one component antioxidant may render the entire antioxidant system less efficient or dysfunctional entirely.
- Due to the high safety and low-cost profile of antioxidant vitamins, nutrients, and the potential clinical utility of this approach, as demonstrated in the case presented here, further clinical research is clearly warranted as this may help many other patients, not only in severe Covid-19, but also other cytokine storm/oxidative stress cases caused by viral or other agents.
Case description: I recently consulted on a Manila (Philippines) Covid-19 patient: Robert, male, 60 years old, he is 176 cm in height (5’9), 90 kg, with type 2 diabetes, hypertension, and with a history of chronic hepatitis B. He developed cough, low fever, and pneumonia on chest X ray. He was admitted to the hospital on 9/1/21 and was given standard therapy. But his clinical conditions didn’t improve and instead worsened. His oxygen saturation went down to as low as 90% and inflammatory/cytokine storm markers were also rising significantly (ferritin rose from 997 on 9/1 to 2202 on 9/6; D Dimer rose from 0.27 on 9/1 to 0.99 on 9/6. His CRP was also very high at 33.97).
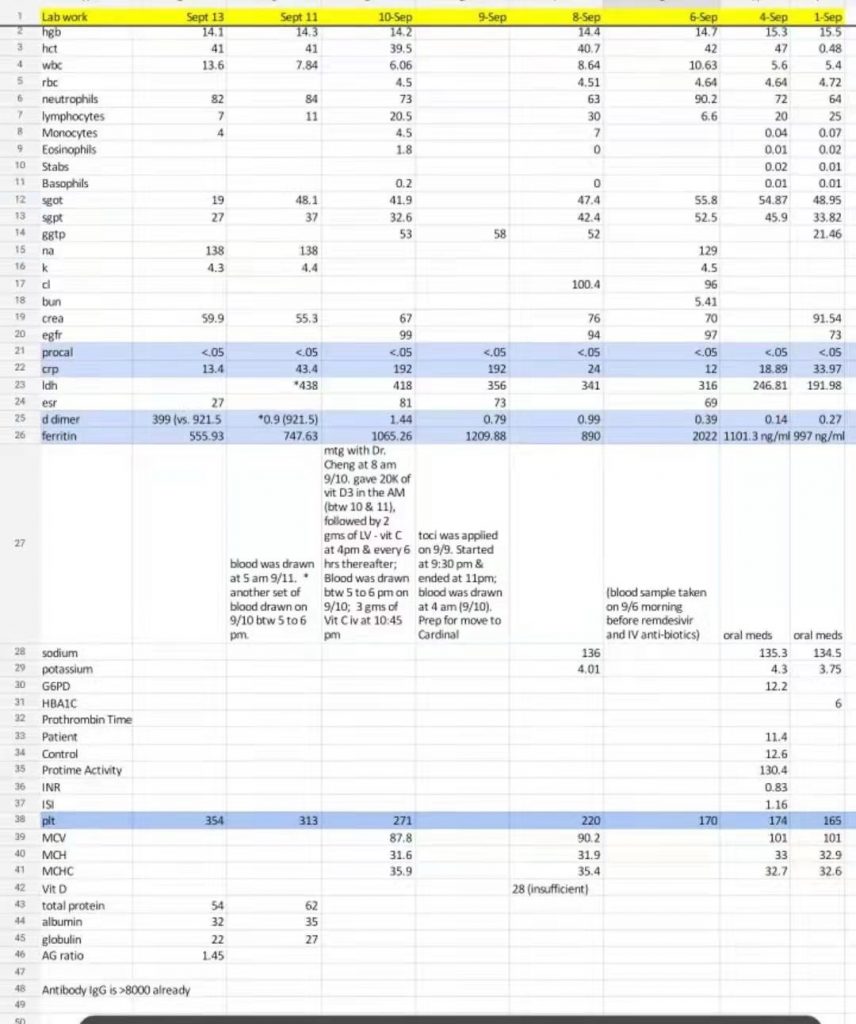 The family requested high dose Vit C (HDIVC), but the attending physician was hesitant due to very high levels of ferritin and also the hospital has a policy on Vit C use of up to 3,000 mg per day.
The family requested high dose Vit C (HDIVC), but the attending physician was hesitant due to very high levels of ferritin and also the hospital has a policy on Vit C use of up to 3,000 mg per day.
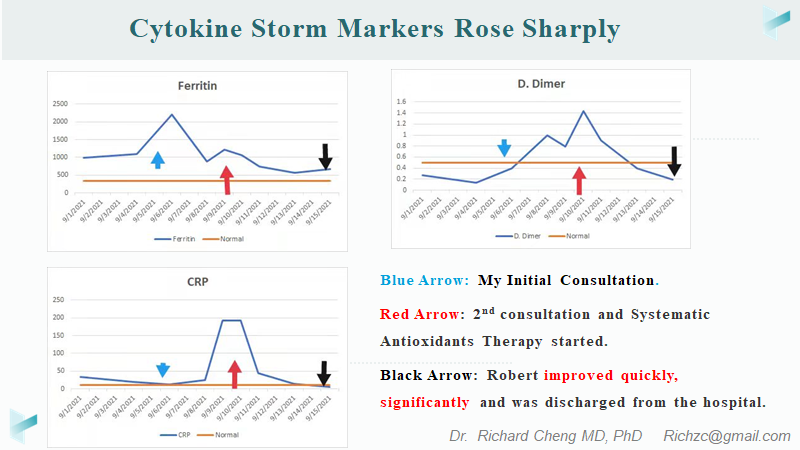
During a video consultation upon request, I pointed out that the poor health status with the comorbidities (diabetes mellitus, hypertension, obesity and active hepatitis B) and the rapidly rising levels of cytokine storm markers, make Robert at very high risk of imminent multi-organ failure and high mortality. The rapidly rising levels of cytokine storm markers suggest that Robert is on the brink of developing cytokine storm, if he is not already in one1–5. The family and the attending are concerned about the high ferritin and the possible side effects of HDIVC. I pointed out Robert’s high ferritin levels are more of an “acute inflammatory” response in nature and a marker for cytokine storm, rather than an indicator of true high iron storage. The priority is to quickly block/control the cytokine storm, to reduce oxidative pressure, to prevent/minimize oxidative damages to the cells, tissues and organs, to prevent multi-organ failure.
I recommend immediate large doses of integrative antioxidant intervention:
- Vit C vein 30 g/24 hours;
- Vit E, 400iu/day 3;
- Vit D3 (his D3 is only 28), 50,000iu, one-time, immediately.
- Magnesium 1000mg/day;
- Zinc 100mg/day x 7-10 days, then reducing to 30-50 mg/day;
- Glutathione (glutathione), 1-2 g/day, intravenous or Lipo, oral
- 3% hydrogen peroxide atomized inhalation, 15-30 minutes, 3-4 times/day (this however, wasn’t implemented due to hospital restriction);
- Other (e.g. CoQ10, alpha lipoic acid, melatonin).
However, due to the policy restriction and other factors, my suggestions weren’t implemented immediately. A few days later, the patient’s condition deteriorated further. Upon the 2nd video consult, I was really worried of an imminent multi-organ failure and was literally begging the attending physician to implement my suggestions. I pointed out loudly the high safety profile of the agents that I recommended with literature references. We, the attending physician, the caring staff, the family and myself worked as a team to figure out a way to implement my suggestions. The hospital limits the maximum amount of intravenous VCs to 3 g/24 hours, so I recommend to give HDIVC at 3 grams/24 hours, and then add liposomal VC (luckily, they were able to find Lipo-VC of LivOn Labs in Manila), 6 grams by mouth as a loading dose and followed by 2-3 grams every 6 hours by mouth. Hydrogen peroxide nebulization, however, was prohibited by the hospital and wasn’t implemented. The rest of my suggestions including Lipo-Glutathione, zinc, high dose Vit D3 were all administered as recommended.
The next day, the patient was beginning to improve, Mike (one of the patient’s brothers) told me. On the third day (September 13th), his clinical conditions as well as his chest R ray showed significant improvement and the oxygen mask was removed. Discharge was planned. On the fourth day after the antioxidants administration (September 14th), the patient was discharged from the hospital to home.
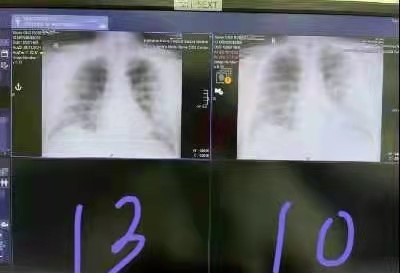
Robert’s Chest X ray on 9/13/21 improved significantly compared with CXR on 9/10/21.
I recommended the continued the integrative antioxidants administration for a few more weeks until clinical and laboratory markers all return to normal and then be placed on a maintenance plan for his chronic disease management. The family scheduled another consultation with me is later for the management of Robert’s ongoing recovery as well as the management of his underlying chronic diseases (diabetes, hypertension and obesity).
On 14 September, the patient was discharged from the hospital and returned home for treatment.
Brief discussion:
Soon after the outbreak of Covid-19, in my paper (3/1/20)4 and in my NIH presentation (4/8/20) 5,6, I (as well as others) pointed out that Cytokine storm/oxidative stress is a key pathological and biochemical feature of severe/critical Covid-19 and other acute respiratory distress syndrome and early and high dose Vit C intravenously should be implemented4. Cytokine storm/oxidative stress is also a common feature of severe cases of influenza7, viral hepatitis8–10, viral encephalitis11, AIDS/HIV12, Ebola13, etc. Oxidative damage of important bio-molecules caused by cytokines storm/oxidative stress is largely responsible for various clinical symptoms of Covid-19.
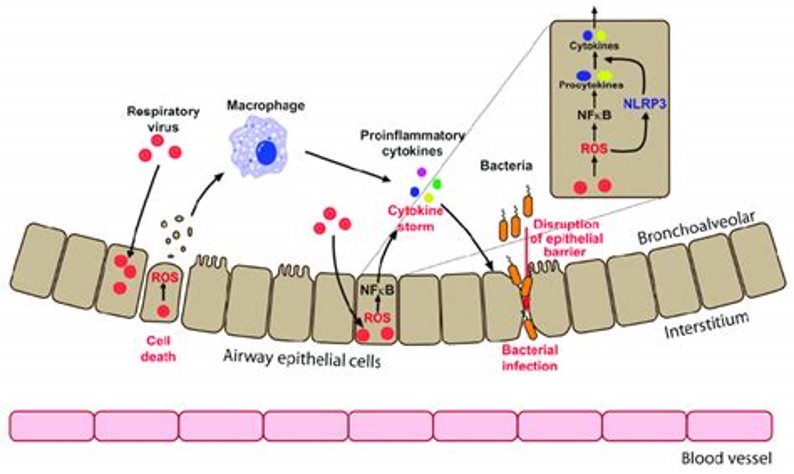
https://www.researchgate.net/publication/326637077_Redox_Biology_of_Respiratory_Viral_Infections/figures?lo=1
Cytokine storm/oxidative stress results in the rapid and significant oxidative damages of bio-important molecules, especially unsaturated fatty acids on cell membranes, in a process called lipid peroxidation chain reaction14–16. This lipid peroxide chain reaction oxidizes PUFA molecules on lipid membranes much more readily and rapidly. The dietary intake of omega-6 PUFA has increased several fold during the last several decades17,18, setting the stage for explosive lipid peroxidation among those with a high PUFA diet. This may be partially the reason of the high morbidity and mortality seen in patients with basic chronic diseases such as diabetes and other metabolic diseases since these patients tend to have a high omega-6 PUFA intake19,20.
There are several different types of oxidants (free radicals) and there are different antioxidant systems that neutralize or scavenge these oxidants21,22. These antioxidants systems require each and every member of a system to be present to be effective. For example, vitamin E is required for the termination of lipid peroxidation chain reaction. In the absence of vitamin E, vitamin C’s is ineffective in termination of lipid peroxidation23.
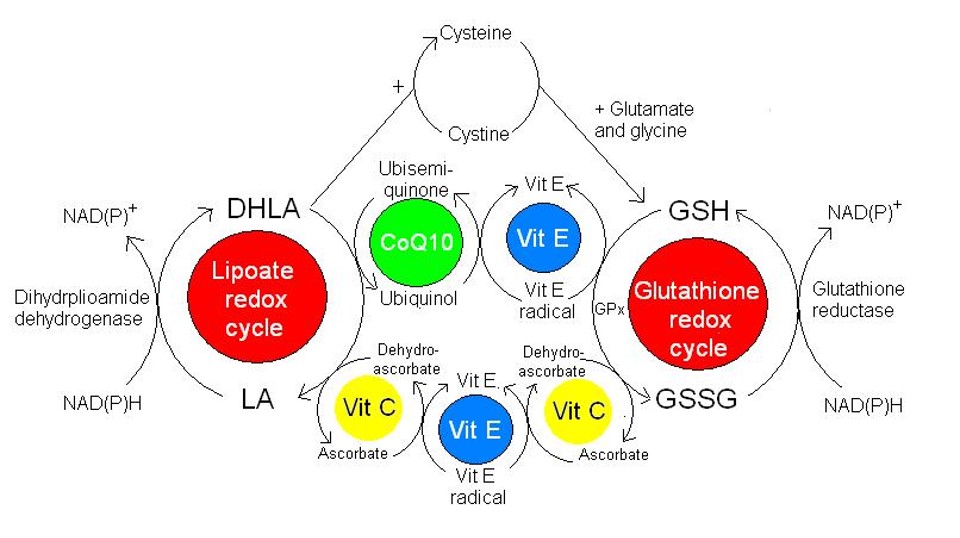
http://www.robertbarrington.net
In conclusion, early and sufficient doses of some basic antioxidants (such as vitamins E, C, CoQ10, glutathione, magnesium, selenium, NAD and NAD precursors) should be systematically implemented in order to prevent or to terminate cytokine storm which may lead to multi-organ failure and ultimately death. In addition to these antioxidants, other agents with natural antiviral or immune boosting effects should also be implemented including, but not limited to vitamin D3, zinc, and hydrogen peroxide nebulization24.
I introduced this concept in my presentation at the 50th Annual Conference of ISOM10.
p.s. This is one of the questions I received from the family:
“Why did Robert’s lungs suddenly improve within 2 days? (On 9/11, the pulmonologist said that Robert needed to be on oxygen for 1 month after discharge. Then on 9/13, after a new X-ray and ABG test, the pulmonologist said he did not need to be on oxygen anymore after discharge. “
References:
- Melo, A. K. G. et al. Biomarkers of cytokine storm as red flags for severe and fatal COVID-19 cases: A living systematic review and meta-analysis. PLoS One 16, e0253894 (2021).
- Huang, I., Pranata, R., Lim, M. A., Oehadian, A. & Alisjahbana, B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther Adv Respir Dis 14, 1753466620937175 (2020).
- Hu, B., Huang, S. & Yin, L. The cytokine storm and COVID-19. J Med Virol 93, 250–256 (2021).
- Cheng, Richard Z. Can early and high intravenous dose of vitamin C prevent and treat coronavirus disease 2019 (COVID-19)? Medicine in Drug Discovery 5, 100028 (2020).
- Cheng, Richard. NIH Guest Speech: HDIVC on Covid-19. http://www.drwlc.com/Covid-19_talks.shtml.
- Cheng, R. Vitamin C in the Prevention and Treatment of Covid-19. (2020).
- Oldstone, M. B. A. & Rosen, H. Cytokine storm plays a direct role in the morbidity and mortality from influenza virus infection and is chemically treatable with a single sphingosine-1-phosphate agonist molecule. Curr Top Microbiol Immunol 378, 129–147 (2014).
- Mbachu, J., Bul, V. & Koppe, S. W. P. The Perfect (Cytokine) Storm: Autoimmune Hepatitis as a Catalyst for Macrophage Activation Syndrome: 1950. Official journal of the American College of Gastroenterology | ACG 111, S930 (2016).
- Xie, J. et al. Cytokine storms are primarily responsible for the rapid death of ducklings infected with duck hepatitis A virus type 1. Sci Rep 8, 6596 (2018).
- Richard Cheng MD PhD. Oxidative Stress, Ignored Key Pathology of Covid-19. (2021).
- Savarin, C. & Bergmann, C. C. Fine Tuning the Cytokine Storm by IFN and IL-10 Following Neurotropic Coronavirus Encephalomyelitis. Front Immunol 9, 3022 (2018).
- Muema, D. M. et al. Association between the cytokine storm, immune cell dynamics, and viral replicative capacity in hyperacute HIV infection. BMC Med 18, 81 (2020).
- Younan, P. et al. Ebola Virus Binding to Tim-1 on T Lymphocytes Induces a Cytokine Storm. mBio 8, e00845-17 (2017).
- Ayala, A., Muñoz, M. F. & Argüelles, S. Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev 2014, 360438 (2014).
- Mylonas, C. & Kouretas, D. Lipid peroxidation and tissue damage. In Vivo 13, 295–309 (1999).
- Ebrahimi, M., Norouzi, P., Aazami, H. & Moosavi-Movahedi, A. A. Review on oxidative stress relation on COVID-19: Biomolecular and bioanalytical approach. Int J Biol Macromol 189, 802–818 (2021).
- Shaikh, S. R. & Edidin, M. Polyunsaturated fatty acids and membrane organization: The balance between immunotherapy and susceptibility to infection. Chem Phys Lipids 153, 24–33 (2008).
- Guyenet, S. J. & Carlson, S. E. Increase in adipose tissue linoleic acid of US adults in the last half century. Adv Nutr 6, 660–664 (2015).
- Muhlhausler, B. S. & Ailhaud, G. P. Omega-6 polyunsaturated fatty acids and the early origins of obesity. Current Opinion in Endocrinology, Diabetes and Obesity 20, 56–61 (2013).
- Knobbe, C. Diseases of Civilization: Are Seed Oil Excesses the Unifying Mechanism?’. (2020).
- Phaniendra, A., Jestadi, D. B. & Periyasamy, L. Free Radicals: Properties, Sources, Targets, and Their Implication in Various Diseases. Indian J Clin Biochem 30, 11–26 (2015).
- Davis, U. 8.1: Introduction to Free Radicals and Antioxidants – Medicine LibreTexts. https://med.libretexts.org/Courses/Metropolitan_State_University_of_Denver/Introduction_to_Nutrition_(Diker)/08%3A_Nutrients_Important_as_Antioxidants/8.01%3A_Generation_of_Free_Radicals_in_the_Body.
- Sato, K., Niki, E. & Shimasaki, H. Free radical-mediated chain oxidation of low density lipoprotein and its synergistic inhibition by vitamin E and vitamin C. Arch Biochem Biophys 279, 402–405 (1990).
- Rapid Virus Recovery: Levy, Thomas E: 9780998312415: Amazon.com: Books. https://www.amazon.com/Rapid-Virus-Recovery-Thomas-Levy/dp/099831241X/ref=sr_1_2?crid=16DCZ0TP1XKB7&dchild=1&keywords=thomas+levy+books&qid=1632088062&sprefix=thomas+levy%2Caps%2C173&sr=8-2.